Safeguarding Reproductive Health
- 说明
子宫粘液中若只有少量血液,可能对你的身体没有害处,它是由于激素水平波动,或者在你怀孕后胚胎移植造成的。但有时候它可能预兆子宫颈或子宫息肉,或者子宫肌瘤,此外还有一些生殖系统的癌症,可能影响你宫颈粘液形态和月经周期。如果在你正常的形态或者正常的月经发生变化,在粘液中出现任何血斑或血迹,请务必告诉你的医生。
宫颈癌
异常出血和阴道分泌物可能是宫颈癌的症状。在“案例研究”一节中我们将提到有一位妇女去就医,检查宫颈粘液的异常形态,结果被诊断为患有宫颈癌。但由于她治疗及时,最后效果非常好。
卵巢和子宫癌
子宫癌的其中一个症状就是阴道分泌物异常,即不同于典型的宫颈粘液。卵巢和子宫癌的症状可能包括月经周期不规则,推迟或者延迟,或者在经期间或更年期后出血。其他症状包括下背部或盆腔疼痛,消化问题,饱胀感和便秘。患有卵巢癌的妇女可能会有腹压和膨胀感以及体重增加。
但务必记住,上述许多症状也可能只是较轻疾病的症状。如有这些症状,请就医检查。及早发现大有裨益!
- 说明
感染
生殖系统发炎是不孕的第二个主要原因。而最主要的原因通常是生殖道感染(通常由性传染病导致)。如果你学会了绘图记录你的宫颈粘液形态,你就能很快地察觉异常,并立即寻求治疗,从而防止生殖紊乱。例如,你可能在你的宫颈粘液中看到少量血迹,或者在有排卵形态的粘液时持续有分泌物。
子宫内膜异位
子宫内膜异位是指患者的子宫内膜长到子宫外部。输卵管、卵巢、泌尿器或肠器官可能会受到影响。此病的诱因尚未知,但其所造成的风险因素可能包括经期提前来临,过敏,肥胖和遗传易感性( genetic predisposition )。
患有此病的女性有30%至40%可能会不孕,因为其生殖器官中存在疤痕。症状有多种,可能包括月经不规则和月经过重,性交疼痛,以及在月经前和月经过程中盆腔疼痛。如果你熟悉你的正常的宫颈粘液形态,就有可能在早期发现这一问题,因为粘液的形态在患此病时可能不正常。
治疗方法可包括激素治疗或手术。通过手术将异位的子宫内膜移除,可能为你的怀孕之旅打开一扇“机遇之窗”。每周进行5个小时的有氧运动可将复发的风险降低一半。分娩也可以极大地降低复发风险。
- 说明
甲状腺异常
一个28岁女性的比林斯排卵期徵状法™图表显示几个月的周期异常,并有过浓的粘液,且无明显的昭示排卵的形态变化。在一个周期中,她出现生殖症状,然后很快就出血,然后又是生殖症状。她的比林斯排卵期徵状法™老师让她到全科医生处检查。孕激素测量确认排卵已开始,但图表明显具有疑惑性。她在过去12个月中曾有过两次流产,并称自己有焦虑、抑郁、疲劳和持续的增重问题。经过检查,发现她有轻微的甲状腺机能减退问题,医生给她开了药。在接下来的几个月中,她的甲状腺刺激素水平恢复到了正常范围,她的疲劳和焦虑问题也有所改观,并且月经周期也渐渐恢复到了正常模式。第二年她怀孕了,并且生下了第二个孩子。
宫颈癌
一个33岁的妇女,应用比林斯排卵期徵状法™已经有一段时间了,通常她绘制的图表都是清晰的粘液形态和规则的月经周期。但在过去两个周期中,她注意到在生殖高峰过后,又有生殖特性的粘液出现。这显然是不正常的,因此她去医院检查。经过早期子宫颈癌涂片检验和活组织检查,确认宫颈腺癌,然后对她进行了全套子宫切除术。幸运地是并没有转移癌的迹象。她的医生说如果她没有在她的图表上发现异常,可能还活不到下一次预定的早期子宫颈癌涂片检验。

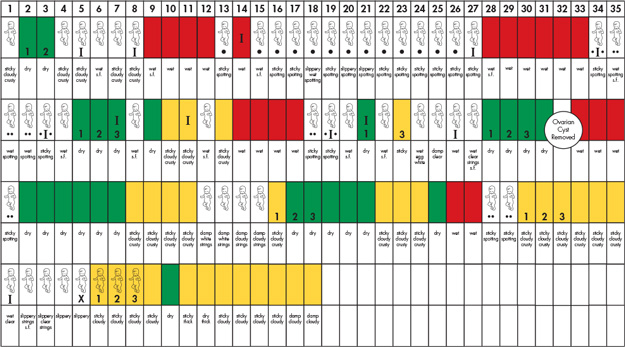
卵巢囊肿
在以下图表中,识别异常出血可及早诊断并成功治疗卵巢囊肿。
- 说明
你可能会想粘液形态和月经周期中哪些不规则情况算是异常。有些卵巢活动是对生活中不同时间和事件的正常反应。你的比林斯排卵期徵状法™图表将会帮助你联系粘液形态和月经周期的变化与你的生活和身体的变化。所以在我们分析什么是异常情况之前,看看哪些是正常的“不规则情况”。
月经开始
当青春期女孩月经初潮时,她们的周期通常不规则,直到其激素形态成熟为止。在前几年里,可能有时候没有卵子从卵巢释放。这种激素活动后的出血可能不规则,时间长并且出血量多。了解排卵可能会延迟几个星期或几个月有助于区分正常和异常情况。研究证明,通过宫颈粘液的形态,青少年女孩可以在排卵时心里有数。如果女孩的周期在两年内都没有达到规则的25-33天,那么她应该去医院检查。
接近更年期
在生殖期限的另一端,接近更年期的妇女也可能会经历月经周期的变化。由于雌激素水平波动,粘液的形态可能变得不规则。排卵延迟,块状粘液和连续出血可能变得普遍。
停止服用激素避孕药
停止服用激素避孕药后你可能在几个星期或几个月内不会出现生殖迹象,直到你的激素恢复正常功能为止。你可能注意到没有定义清楚的粘液形态,表示你尚未开始排卵,或者子宫颈还没有从避孕药的影响中恢复过来,还没有开始产生具有生殖能力的粘液。如果你正计划怀孕,研究表明,在停药后的三个月内,受孕率较低,有时候这种情况会一直持续到第十个月。但每一位女性都是独特的。你的生殖能力可能会很快恢复,可能在停药后的几周内就能怀孕。在图表中记录你的粘液形态有助于你跟踪正在恢复的生殖力。
如果你正计划怀孕,建议你开始服用叶酸(Folic acid)补充剂,最好是在你怀孕前的几个月内服用。
哺乳
生育后,你的生殖能力要完全恢复需要数周或数月的时间。如果你采用母乳喂养,可能会注意到需要很长时间才能恢复到规则的月经周期。当然也有即便你是在哺乳期,可能在生育后的几个月内你就恢复了生殖力。每一位女性都是不同的。
其他事件
长途旅行,激素治疗,激素避孕药,劳累的体力活动,大幅度增重或减重,压力和疾病都能扰乱你的激素水平,导致你的宫颈粘液形态和月经周期发生变化。
如果你的图表显示出你无法解释的异常模式,你可能出现了激素紊乱或其他需要进一步检查的问题。下一节介绍正常的出血类型,然后我们再探讨宫颈粘液形态或月经周期的不正常现象。
- 说明
排卵功能障碍是指无排卵或排卵活动异常。此情况是不孕的主要原因。它通常与月经周期不规则有关,一般由激素紊乱导致。例如:
多囊性卵巢综合征
肾上腺激素和卵巢激素异常是卵巢功能障碍的最常见诱因,最常见的例子是多囊性卵巢综合征(PCOS)。据估计,约有5%-10%的澳大利亚妇女患有PCOS,但许多人对自己身患此病并不知情。通常患有PCOS的妇女有抗胰岛素性,导致高胰岛素水平。其卵巢和肾上腺也可产生过多的睾丸激素。这种激素失调意味着内含发育中的卵子的卵泡不能适当地成熟。通常卵子不会被从卵巢释放,因此无排卵。挣扎中的卵泡继续生成更多的睾丸激素,从而影响排卵过程。很快许多这样的小囊就会覆盖卵巢。
如果你患有PCOS,第一次开始月经后,你可能会有不规则的周期。其他症状可能包括粉刺,多毛,体重增加,但有些妇女可能没有任何症状。在绘制图表的过程中,你可能会注意到持续的表明具有生殖能力的粘液形态,或者数天的粘性或湿滑粘液逐渐演变为生殖高峰。
若被诊断为患有PCOS,医生可能会开避孕药,以便诱发规则的每月出血。但避孕药只是治标不治本。例如,服食避孕药不能解决抗胰岛素的问题,抗胰岛素性会增加患糖尿病的风险。应该测量胰岛素和血糖浓度,医生可能会建议通过药物、饮食和运动来治疗抗胰岛素性。限制胰岛素水平和恢复血糖平衡也有助于控制睾丸激素的产生。这将有助于恢复正常的排卵和规则的月经周期。
绘制周期和宫颈粘液形态的图表有助于你的医生诊断病情,并计划你的治疗方案。如果你尝试怀孕,图表将有助于你识别哪些周期可能有生殖力。饮食、锻炼和医疗将有助于你恢复到正常的卵巢活动。
比林斯排卵期徵状法™的老师会教你理解你的图表,并在必要时建议你寻求医生建议。
其他激素紊乱问题
高催乳素血症:泌乳刺激素是一种与哺乳相关的激素,但有时在服用某些药物后,或由于垂体瘤或激素失调(如甲状腺机能减退),此激素的浓度会过高。过量的泌乳刺激素会干扰控制卵泡生长的激素。具有此激素紊乱问题的妇女可能根本没有月经,出血不规则或者月经周期短(有经前血斑)。高催乳素血症可以用药物治疗。
甲状腺机能亢进/甲状腺机能减退:甲状腺激素水平过高的女性可能会有月经周期不规则的问题(月经时间间隔长),以及异常的轻微出血。甲状腺激素水平过低的女性可能经历不规则出血问题(出血量过大,时间长)。在“案例研究”部分你将看到有一位妇女通过宫颈粘液形态异常问题察觉出了甲状腺异常。
- 说明
比林斯排卵期徵状法™不仅仅适用于希望怀孕或避孕的女性。它是每一位妇女都需要掌握的知识。为什么呢?因为它能帮你保障自己的生殖健康。
比林斯排卵期徵状法™图表具有诊断作用
宫颈粘液的变化可以准确地反映你的生殖激素正在发生什么变化。这张图表保存起来可以准确地记录这些激素情况。50多年的研究和激素分析证明了这一点。
“粘液的产生可以用来对卵巢激素生成进行自我分析”
James B. Brown,妇产科教授
一旦你了解了什么是正常现象,你就能判断出异常。如果你在你的模式中注意到不规则情况,例如异常出血或异常分泌物形态,你就知道如何去检查这些情况。你的医生可以使用你的图表帮助诊断问题,并为你提供最佳治疗方案。
如果你因为产科问题,比如月经周期不规则,去看过医生,很有可能医生会给你开避孕药。避孕药可能会使你的周期变得规则,但这只是治标不治本,因为没有诊断或治疗潜在的诱因。
当你使用比林斯排卵期徵状法™绘制你的宫颈粘液形态时,你将可以给你的医生提供有价值的信息,帮助他/她诊断你的症状的潜在诱因。
比林斯排卵期徵状法™
- 让你掌控自己的身体。它能让你积极地管理自己的生殖健康。
- 让你以一种很实用的方式理解你的身体。它教会你识别任何可能需要及早就医的变化。
- 适合你自身独特的生殖和非生殖模式,这样你就能够判断出正常和异常情况。
继续阅读,了解你在生活中不同时间可能看到的正常的“不规则情况”,然后我们会介绍比林斯排卵期徵状法™如何帮你识别异常情况和需要检查的情况。
学会如何绘制比林斯排卵期徵状法™图表很简单。
从今天开始,保障你的生殖健康!
拨打1800 335 860与我们约见。如果你无法前往我们的辅导中心,我们可以通过电话给你指导。
- 说明
月经
子宫衬里,称为子宫内膜,在每个月经周期会因雌激素而增厚。孕激素水平在排卵时开始上升,使子宫内膜发生变化,从而为受精卵的移植做好准备。如果没有怀孕,孕激素和雌激素水平会下降,导致子宫内膜脱落。
雌激素突破性出血
雌激素上升时子宫内膜都会作出反应。雌激素突破性出血是由于雌激素浓度高导致的,有时候在卵泡排卵之前发生。或者卵泡可能没有发育完全,还处于慢性刺激状态,因此子宫内膜继续形成;当子宫内膜的生长速度超过供血速度时,突破性出血就会发生。
突破性出血表明可能具有生殖力,并且可能与其他症状相关,如可见的粘液或湿滑感。出血可能时间长,且量多,也有可能只是一两天的少量出血或血斑。
雌激素撤退性出血
当内含卵子的卵泡中开始发育时它会产生雌激素,从而导致子宫内膜开始增厚。但有时卵泡不能完全成熟,因此无排卵。卵泡破裂,导致雌激素水平下降,子宫内膜没有雌激素的支持,从而可能发生出血。这种出血可能量大,甚至有血凝,可能持续一段时间,也可能较轻微或只有血斑。
雌激素撤退性出血和突破性出血可能发生在雌激素水平波动的时候,例如在青春期,哺乳时,停止激素避孕药时以及接近更年期时。如有疑问,请咨询你的比林斯排卵计算法TM老师,她会建议你是否就不明的出血寻求医护。
胚胎移植
这可能发生在怀孕一周后,此时受精卵移植到了子宫内膜中。
任何原因不明的出血都应该检查。下一节我们谈一谈需要检查的宫颈粘液和月经周期异常。
WE'RE JUST A PHONE CALL OR CLICK AWAY!
Contact us to set up an in-person or online appointment with an accredited Billings Ovulation Method® tutor who will guide you through each step of the process.
Your personal tutor is here for you to help you and answer
all your questions along the way!
DONATE to Billings LIFE - Leaders in Fertility Education



")
")
")